

In Part 3 of this series on Vitamins, Minerals, and Nutritional Supplements, we will explore some of the dietary supplements used by athletes to improve performance. Future articles will continue this discussion, as a full discussion of all of them would require a very long article. In addition, many semi- and non-athletes may use these products as well.
These articles are designed to provide information about supplementation so that the reader understands what the state of legal supplementation is like. Another one for those of us weekend warriors or other athletes not connected to the elite training that Duck athletes receive, this article about the Terry Crews workout routine and diet plan, and others like it, in the past and to come, will educate us as to how best to keep our bodies healthy and prepared for exercise and sports.
|
‘Buyer Beware’ Information about Supplementation |
Most supplements are not tested adequately for efficacy, purity, or safety. |
Be careful of misleading product information. |
‘Natural’ does not mean safe! |
‘More’ is seldom better! |
Nothing replaces a well-balanced diet that includes a variety of high-quality foods with plenty of nutrients. |
Athletes, and others, use supplements at their own risk! |
Commonly Used Athletic Performance Supplements
The optimal and long-term side effects (also, ‘adverse effects’ – we will use both terms interchangeably in this article and its sections) of most supplements are not known. Manufacturers recommend doses and durations that have been tested, and claimed side effects apply to these instructions. Many athletes may use higher doses than recommended and/or use them for longer periods of time, which raises concern for unknown effects, as well as for more severe adverse effects. Most supplements try to enhance the normal effects of exercise on the body.
Arginine:
Claims: Arginine is said to acutely improve exercise capacity. Its chronic effect results from the stimulation of muscle protein synthesis and thus, anabolism (the synthesis in living organisms of more complex substances (e.g., living tissue) from simpler ones together with the storage of energy) of muscle protein. Soy protein is an excellent source of arginine.
Mechanism: Arginine may promote secretion of endogenous (derived or originating internally) growth hormone (GH). It is a precursor in the synthesis of creatine (see section below on creatine). It augments the production of nitric oxide (see section below on Nitrous Oxide).
Efficacy: There is little scientific evidence available to support the claims of promoting and increasing functional capacity in healthy athletic participants. Intravenous arginine (medicine administered from a drip, down through a hollow needle inserted into a patient’s vein) does increase GH, but oral ingestion has not shown the same effect. Arginine may increase nitrous oxide (NO) production, but definitive studies have yet to be done. One condition has reliably responded to arginine supplementation. It is with inborn errors of urea (the chief solid component of mammalian urine) synthesis. Other conditions that need more studies to confirm efficacy include heart disease, heart failure, and peripheral vascular disease. Other medical conditions’ responses are inconclusive.
Side Effects: Arginine may cause bloating; diarrhea; endocrine changes; gastrointestinal discomfort; hives; increased blood urea nitrogen, serum creatine, and serum creatinine; increased inflammatory response; leg restlessness, lower back pain; nausea, numbness (with arginine injection); rash; reduction in hematocrit; severe tissue necrosis with extravasation; systemic acidosis; or venous irritation. In heart disease patients, arginine may cause high white blood cell count, increased post-heart attack deaths, lack of energy and strength, and vertigo or increased blood pressure (in heart transplant patients).
- Arginine may increase the risk of bleeding.
- Use cautiously in patients with impaired kidney function or those at risk for hyperkalemia (abnormally high levels of blood potassium), including those with diabetes or using drugs that elevate potassium levels, such as potassium-sparing diuretics and potassium supplements, as arginine may cause hyperkalemia. Fatal cardiac arrhythmia occurred in one patient.
- Use caution with phosphodiesterase inhibitors (e.g., sildenafil [Viagra®]), due to a theoretical risk of additive blood vessel widening and blood pressure lowering.
- Use with caution in postmenopausal patients, as night sweats and flushing have been reported.
- Use with caution in patients with herpes virus, as L-arginine may worsen this condition. L-arginine may increase the risk of herpes simplex cold sores.
- Use with caution in individuals at risk for headaches, as headache has been a reported side effect. In mountain climbers, L-arginine increased the risk of developing a headache.
- Use with caution in patients with immunological disorders.
- Use cautiously in patients with sickle cell anemia as arginine may cause worsening of symptoms.
Dosage: There is no current suggested daily intake or tolerable upper intake for arginine. This amino acid is considered nonessential. The therapeutic dosage (maximum dose considered safe) is 400-6,000 mg (1 gram=1000 mg).
Bovine Colostrum (BC):
Claims: Some claim that bovine colostrum supplementation increases insulin-like growth factor-1 (IGF-10 levels. BC supplementation appears to positively influence exercise performance characterized by short bursts of activity. In elite-level athletes, supplementation has not been found to improve body composition. In non-athlete athletes, body composition improves. Bovine colostrum has been used to treat diarrhea, to improve GI health, to boost the immune system. Several athletes have used bovine colostrum supplementation for the benefit of being healthier during training and in-season competition. Interestingly, a banned substance in some sports is deer antler velvet, one of the purest known sources of IGF-1.
Mechanism: BC stimulates growth factors, including structurally IGF-1. IGF-1 has an anabolic effect (promoting constructive metabolism) and is involved in the regulatory negative feedback of growth hormone. GH stimulates hepatic (liver) production of IGF-1. As IGF-1 levels rise, they provide negative feedback to inhibit the pituitary gland’s production of GH.
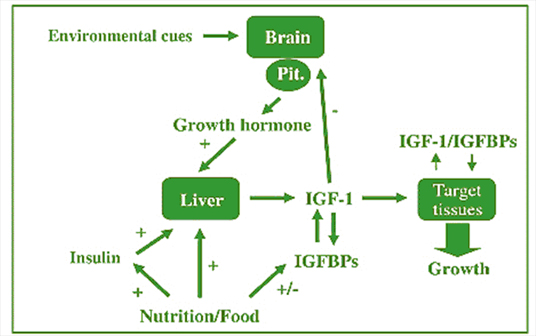
IGF-1 negative feedback loop. Note the role of the environment and nutrition
Efficacy: Bovine colostrum contains greater levels of some factors than does human colostrum in mother’s milk. This fact is especially important for the immunoglobulin (a protein that acts as an anti-body) called IgG. While human colostrum contains only 2 percent of this critical immunoglobulin, bovine colostrum contains up to 38 percent. IgG is considered to be one of the body’s most important immunoglobulins, because it is active against so many different microorganisms, many of which are now resistant to antibiotics now on the market. The increasing inability of antibiotics to fight common and often deadly microorganisms makes the use of colostrum of paramount importance in the fight we cannot afford to lose. Therefore, in a sense, Bovine colostrum is even better for one than human colostrum.
Immunoglobulins are of critical importance because bacteria are becoming increasingly resistant to antibiotics. New viruses are multiplying and mutating faster than the vaccines to combat them. Moreover, bacterial and viral infections are being linked to more diseases (e.g. cancer, peptic ulcers, and heart disease). In fact, the relationship between bacterial infection and heart disorders has strong evidence to support it. Colostrum and its rich supply of Immunoglobulins (cytokines, PRP, Lactoferrin and other immune factors) may play a major role in combating this serious health problem (it is the number one cause of death).
Immunoglobulins in bovine colostrum provide unique protection against virtually all disease causing organisms. In addition, it is unique because the levels of immune factors in bovine colostrum are 10 to 20 times greater than that found in human colostrum.
Your body can make good use of those immunoglobulins. The majority of immunoglobulins are manufactured in the bowel. Bovine colostrum delivers its immunoglobulins to the bowel. It is a perfect match.
It is useful here to mention that the immune system and immunoglobulins influence moods, behavior, and functioning, and are in turn influenced by behavior, moods, emotions, and bodily functioning, in turn.
Side Effects: Human colostrum is very safe and has no side effects (it is found in mothers’ milk).
On the other hand, bovine colostrum has a side effect known as the “healing crisis.” Healing crisis occurs when the cells release toxins stored in them. Symptoms of healing crisis include headache, upset stomach, nausea, diarrhea, cough, rash, mild fever, and bloating. The usual daily dose of the commercially available BCC preparation, LactobinA (LC1) is 10-20 g daily, but higher doses can be used in the majority of patients because of the low incidence of intolerance problems.
Importantly, in several well-done studies, there were no cases of BSE-associated disease such as the new variant of Creutzfeldt-Jakob disease with the use of bovine colostrum. Bovine spongiform encephalopathy (BSE), also known as ‘mad cow disease’, and variant Creutzfeldt-Jakob disease (CJD) are related disorders (also called ‘prion’ diseases). They belong to the family of diseases known as the transmissible spongiform encephalopathies (TSEs). TSEs are caused by a transmissible proteinaceous particle, which is yet to be fully characterized. Other TSEs include scrapie (a disease of sheep), feline spongiform encephalopathy, transmissible mink encephalopathy, and chronic wasting disease of deer and elk. Human forms include classic CJD, variant CJD, kuru, Gerstmann-Sträussler-Scheinker disease, familial fatal insomnia, and sporadic fatal insomnia.
A high percentage of participants in studies complained about the unattractive taste of the beverage. Presumably, available commercial preparations deal with this aspect.
Dosage: 20-60 grams/day.
Branched-Chain Amino Acids (BCCAs):
Claims: BCCAs are an important source of energy in prolonged endurance exercise. Supplementation is proposed to increase endurance in long tennis matches, soccer, marathons, long-distance swimming, and cycling activities. BCAA supplementation may contribute to increased body fat loss and maintenance of a high level of exercise performance. BCAAs are also claimed to decrease chronic fatigue/over-training symptoms (washed-out feeling, tired, drained, lack of energy, mild leg soreness, general aches and pains, pain in muscles and joints, sudden drop in performance, insomnia, headaches, decreased immunity [increased number of colds, and sore throats], decrease in training capacity / intensity, and moodiness and irritability).
Mechanism: Supplementation replenishes loss of BCAAs used as fuel, increases protein synthesis and growth hormone secretion, shifts leucine metabolism to fat metabolism, stimulates fat metabolism over glycogen in hypocaloric diets (low calorie), and prevents the decrease of plasma glutamine. BCAAs inhibit dietary tryptophan transport across the blood-brain barrier leading to decreased brain serotonin (tryptophan is the precursor for serotonin). This is associated with several brain regions that control central fatigue.
Leucine, which is at the center of the mechanism of BCAAs, is an essential amino acid (amino acids can be classed as either ‘essential’ or ‘non-essential’). Essential amino acids are those that must be consumed in the diet because the body cannot synthesize them. Of the eight generally-termed essential amino acids, the three “branched chain amino acids” – isoleucine, leucine and valine – are often considered to be the most important, especially in relation to exercise.
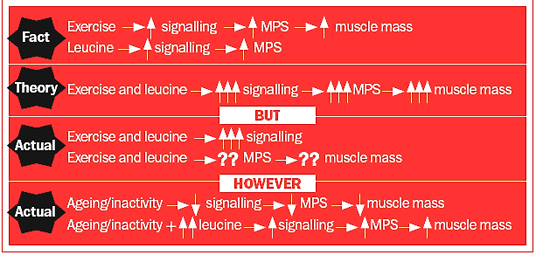
Summary of what is known and what is speculated about the mechanism by which BCCA-leucine (an amino acid) results in increased muscle protein synthesis and muscle mass in healthy, young adults and in the elderly and inactive.
MPS=Muscle Protein Synthesis; ↑=increase; ↓=decrease
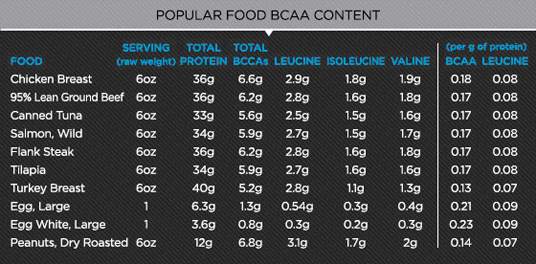
Foods with relatively high BCAA content
Efficacy: Most studies show neither beneficial nor detrimental effects of BCAAs. Studies of the effect of BCAAs in the hypocaloric state are limited. BCAAs have not been shown to reduce chronic fatigue/over-training symptoms.
To complicate the situation further, most studies demonstrating a beneficial role of supplemental BCAAs used untrained individuals; the implications of these findings to athletes are therefore currently unknown. Moreover, BCAAs can be found in a number of foods in relatively high amounts, and so supplements may not be necessary at all.
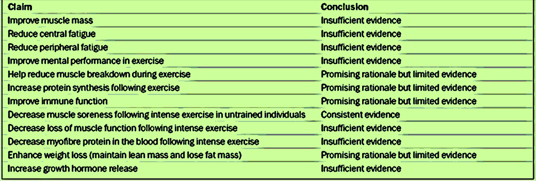
Claims for BCAAs and research conclusions
More studies are needed to determine the effectiveness of BCAA supplements for athletes and women. Consequently, caution is warranted before accepting the vast majority of the claims on websites, advertisements and labels. In addition, many claims are based on animal studies (usually rats), and not on humans. Look for this distinction if you want to do your own research on this matter.
Side Effects: Fatigue and ergolytic effects (pertaining to any substance that impairs exercise performance) have been reported.
Dosage: Usually combined with other amino acids. The range: 5 to 10 grams/day or before exercise.
Carbohydrate Supplements:
Claims: Carbohydrate supplements are used to restore muscle glycogen after exercise, maintain plasma glucose during endurance events (especially those lasting more than 90 minutes), and to maximize muscle glycogen before significant glycogen-depleting exercise (e.g., marathon, long course triathlon). Various sugars are used, including sucrose, glucose, and maltodextrin (popular among ultra-endurance athletes).
Mechanism: Increased blood glucose stimulates insulin production and GLUT-4 translocation (an exchange of chromosome parts) in muscles, which results in increased glucose uptake (into cells) and glycogen storage in muscle (insulin puts glucose into cells from the blood, and glycogen removes it for use). Carbohydrates with a high glycemic index increase plasma glucose quickly and serve as a fuel source in sustained exercise.
Efficacy: Reviews are mixed for pre-exercise supplementation and carbohydrate loading (a dietary practice of some endurance athletes, such as marathon runners, intended to increase glycogen stores in the muscle tissue). The original, or “classic,” carbohydrate loading regimen began with a period of several days on a low-carbohydrate diet designed to deplete stored glycogen, followed by consumption of a diet high in complex carbohydrates for three days before the event. A more modern approach advocates that athletes routinely consume the high-carbohydrate diet recommended for the general population (55 to 60 percent of total calories), and eat extra carbohydrates (70 percent) for three days before an event.
The practice is controversial and is not universally accepted. Carbohydrate loading prior to endurance events has been demonstrated in literature to be a valuable tool for athletes competing over longer times and greater distances. Techniques range from improved training methods, one to six days of carbohydrate loading, to carbohydrate supplementation during endurance events. No matter which technique is used, it is important to know that when muscle glycogen levels are depleted, the fatigue that sets in is irreversible during the event.
Benefits of supplementation after exercise and during long-events (more than 90 minutes) are well supported by research.
Side Effects: Although carbohydrate ingestion can improve exercise performance, consuming large amounts of carbohydrate is not necessarily a good strategy. Carbohydrate from a drink or food will spare liver glycogen, increase carbohydrate oxidation by muscle, and positively affect certain central nervous system responses, but ingesting too much carbohydrate can have detrimental effects. Highly concentrated carbohydrate solutions and drinks with high osmolality have been linked to the development of gastrointestinal discomfort. A balance must be found between ingesting optimal levels of carbohydrate, which can be oxidized for energy, and avoiding GI discomfort that can lead to poor performance. Otherwise, no other side effects have been noted.
Dosage: 0.7 to 10 g/kg every two hours for the first four hours after exercise (first 90 minutes post-exercise is most important). Best if started within 30 minutes of stopping exercise. Use a food source with a high glycemic index (an indicator of the ability of different types of foods that contain carbohydrate to raise the blood glucose levels within 2 hours. Foods containing carbohydrates that break down most quickly during digestion have the highest glycemic index. Also called the dietary glycemic index). The addition of protein to a carbohydrate supplement increases glycogen production.
During exercise: .7-1.0 g/hour for events lasting more than one hour. Sources include sports drinks (5-10 fl.oz. every 15 minutes), sports gels or candies (two gels and water), or gummy candy (a handful/hour and water). Before exercise, (benefits of carbohydrate loading is controversial): 4 g/kg within three hours before and 1.1. g/kg I hour before; 10 g/kg/day of carbohydrates three to seven days before the event.
Chromium:
Claims: Chromium is a trace mineral that is used for weight loss and for enhancement of glycemic control in the treatment of diabetes. It has been proposed for the treatment of hyperlipidemia (an excess quantity of lipid in the blood) and hypercholesterolemia (an excess of cholesterol in the blood). Athletes use it in attempts to gain muscle and lose fat.
Mechanism: Chromium functions in carbohydrate, protein, and fat metabolism as a co-factor that enhances the action of insulin (to store glucose in cells as fat) and the uptake of amino acids into muscles. It improves lipid profiles, and is theorized to sensitize insulin receptors in the brain. This results in appetite suppression and down-regulation of insulin secretion. Glycogen synthesis increases in chromium-deficient individuals. Exercise may result in loss of chromium, but athletes conserve chromium and probably do not become deficient.
Efficacy: Chromium picolinate is possibly effective when used to reduce cholesterol, but is probably ineffective for weight loss. Mild hypoglycemic effect (low blood sugar) is caused by a mechanism similar to metformin (used to treat high blood sugar levels that are caused by a type of diabetes mellitus or sugar diabetes called type 2 diabetes). A large body of scientific evidence indicates that chromium has no effect on body composition when taken in supplement form, and there are serious concerns for the potential adverse effects of chromium accumulation in the human body.
Side Effects: Chromium interferes with iron metabolism (used for hemoglobin in red blood cells) and zinc absorption. Prolonged use and abuse are linked with serious adverse effects, including anemia, chromosomal damage, cognitive impairment, interstitial nephritis (Interstitial nephritis is a kidney disorder in which the spaces between the kidney tubules become swollen (inflamed). This can cause problems with the way the kidneys work), and gastrointestinal (GI) intolerance. Commercial products containing ephedrine recently have been restricted. Low doses of the combined preparation have been found to cause hypertension, stroke, and even death. If one must use chromium picolinate, make sure that nothing else has been added.
CREATINE: Creatine is probably the most often used and the most researched supplement taken by athletes.
Claims: Creatine is said to increase exercise performance in short repetitive bout of high-intensity exercise offset by brief rest periods (30-120 seconds). This increase in exercise performance and work capacity probably leads to increased muscle mass in some athletes.
Mechanism (postulated): Creatine is a low molecular weight, complex amino acid and is produced endogenously (from within the body) primarily in the liver and stored principally in skeletal muscle. Hydrolysis (the process by which chemical compounds are broken apart by the addition of water – the digestion of food is an example of hydrolysis, as water helps to break down the compounds one has eaten) of creatine phosphate results in rapid production of ATP which is needed for muscle contraction. One can find in the first nutrition article a discussion of ATP in energy production. Maximal muscle stores of total creatine may enhance the ATP turnover rate and increase phosphocreatine resynthesis (a second or subsequent synthesis, especially one using components that were originally combined and broken down), resulting in shorter recovery periods and overall increased training load (volume/intensity). Creatine depletion is the limiting factor in anaerobic exercise (e.g., isometric exercises are anaerobic). Free creatine may stimulate protein synthesis and cause muscle hydration, which results in increased muscle mass and strength.
Efficacy: Numerous studies have examined the effect of creatine supplementation on athletic performance. Despite some disagreement, the consensus is that such supplementation has a small, but real, beneficial effect on anaerobic activity, specifically short duration, repetitive, high-intensity exercise. It does not benefit aerobic training or performance (e.g., running is aerobic). Data about chronic creatine supplementation, high-dose supplementation, and supplementation in young athletes are lacking. There also appear to be responders and non-responders to creatine. Specifically, vegetarians who do not ingest primary exogenous (produced outside the body) sources of creatine (meat and fish) may benefit more from supplementation.
Side Effects: No serious side effects of have been consistently documented from creatine supplementation. Weight gain is a proven side effect, however. Areas of theoretical concern and anecdotal reports (based on incidental observations or reports rather than systematic evaluation) include the following:
- Renal: Creatine is spontaneously degraded to creatinine, and increases in both urine and plasma creatinine levels have been reported. People with a history of kidney dysfunction or disease (e.g., diabetes) that may lead to renal malfunction should approach creatine use with great care and should consult their doctor before using it at all. Additionally, athletes using potentially nephrotoxic drugs (poisonous to kidney tissue – e.g., NSAIDS) may be at higher risk of renal dysfunction. Close monitoring of creatine on the kidney should be considered. Long-term effects of creatine on the kidneys are unknown, but caution must be used.
- Gastrointestinal: Nausea, bloating, cramping, and diarrhea have been described in creatine users. However, such effects are not supported by studies (studies are based on statistical analysis and do not necessarily suggest that these effects are not found in some patients, but that they are just not found in sufficient numbers of people to count as having reached a statistical level of proof in large groups of patients).
- Cardiovascular: It is unknown how much creatine uptake there is by the myocardium (the middle of the three muscle layers forming the wall of the heart). Animal studies that report no substantial myocardial uptake also report no skeletal muscle uptake. Whether this means that skeletal muscle uptake might suggest myocardial uptake is unknown. It appears not to cause hepatic (liver) dysfunction.
- Dehydration (also see section about fluid replacement beverages for more about dehydration, how to gauge it, and how much to drink): Because of anecdotal reports of dehydration, especially in hot, humid conditions, creatine users should take measures to ensure adequate hydration. The patient in this condition is not truly ‘dehydrated’. Total body water is actually increased. However, the osmotic properties of creatine (relating to diffusion of molecules through a semipermeable membrane from a place of higher concentration to a place of lower concentration until the concentration on both sides is equal) can increase third spacing. This is the shifting of fluid from the intravascular space (the inside of a blood vessel) to a nonfunctional space (e.g., abdomen or thorax). This depletes intravascular fluid volume. This causes an increase in the blood levels of nutrients, supplements and medications, and glucose and inefficient distribution of oxygen. An increase of blood sugar will make it harder to prevent some of it being stored as fat. It also means that medications (including pain medicines and NSAIDs) will be closer to toxic levels and can therefore more quickly cause harm. Thicker blood is harder to push along arteries and veins. It increases blood pressure, puts extra burden on the heart and kidneys, and means that glucose and oxygen timing will be a dysfunctional (i.e., not reaching where they are needed in the brain and body when they are most needed – a timing problem). It will also make the removal of toxins from the body, through the kidneys and the liver, less efficient. All of this will result in the body working inefficiently, and performance will suffer.
- Muscular: Anecdotal reports have led to the widespread belief that creatine can induce muscle cramping. This effect remains unproven, although one can see how it could happen: if one’s liver stops working properly (see above section), toxins will build a dose of medication, often larger than subsequent doses, administered for the purpose of establishing a therapeutic level of the medication in your blood, which can make muscles go into spasm. Anecdotally reported muscle strains occur. Fluid retention that may accompany creatine ingestion, especially with loading doses may theoretically increase compartment pressures and predispose an athlete to exertional compartment syndrome (chronic exertional compartment syndrome is an exercise-induced muscle and nerve condition that causes pain, swelling and sometimes even disability in affected muscles of the legs or arms.
- Anyone can develop chronic exertional compartment syndrome, but it is more common in athletes who participate in sports that involve repetitive impact exercise, such as running and fast walking.
Dosage: Some recommend loading doses (a dose of medication, often larger than subsequent doses, administered for establishing a therapeutic level of the medication) of 20-30 grams/day (5-7 grams four times daily) for 5-7 days. This an amount of creatine equal to the amount of five to six pounds of beef (it is best to get your normal levels of creatine from your diet…beef is not the only source). If using loading for creatine supplementation, use doses of 2-4 g/day to maintain intramuscular creatine stores.
Other investigators have found that intramuscular creatine stores reach the same level with 3 g/day and that stores are maintained with as little as 2 g/day of creatine. This approach eliminates the loading phase. It also means that proper diet practices can do this maintenance.
Fluid Replacement Beverages:
Claims: Fluid replacement beverages are used to prevent and treat dehydration. If one exercises in any activity that makes people sweat, one needs to drink extra water to compensate for the fluid loss. An extra 400 to 600 milliliters (about 1.5 to 2.5 cups) of water is sufficient for short bouts of exercise below 40 minutes. However, intense exercise lasting more than an hour requires more fluid depending on how much one sweats during exercise, and the duration and type of exercise. Sipping fluids every 10-15 minutes is a good rule of thumb.
The single best way to determine how much post-exercise fluid a person requires is done by weighing (without clothes) before and after hard exercise. A drop in body weight of 1 kg equates to 1 liter of water required to regain the individual hydration norm. However, one should not drink it all at once, but slowly consume it over the post-exercise hour.
Sports drinks have electrolytes (and generally carbohydrates) within them, which are beneficial during and immediately after intense or prolonged exercise as they aid increased fluid absorption and give carbohydrate energy back to fatigued muscles.
There are three types of sports drinks:
- Isotonic drinks, which quickly replace fluids lost by sweating and supplies a boost of carbohydrate. This drink is the choice for most athletes.
- Hypotonic drinks, doing the same job as isotonic drinks but without the added carbohydrate.
- Hypertonic drinks: used to supplement daily carbohydrate intake normally after exercise to top up muscle glycogen stores. In ultra-distance events, high levels of energy are required and hypertonic drinks can be taken during exercise to meet the energy demands. If used during exercise hypertonic drinks need to be used in conjunction with isotonic drinks to replace fluids.
Sports drinks contain citric acid; which have an erosive potential on teeth so brushing after use and regular use of a neutralizing mouthwash is a good idea.
Researchers used to believe that caffeinated drinks had a diuretic effect. This means that you would urinate more after drinking them, which could increase the risk of dehydration. Recent research however shows that this is not true and that caffeine has a diuretic effect only if one consumes large amounts of it: more than 500 to 600 milligrams (five to seven cups of coffee) a day.
So, carry that water bottle around with you during the day, keep a bottle on your desk – but make sure you actually drink them, each day, and try the following strategies to increase your daily fluid intake;
- Have three pieces of fruit each day
- Have three (especially green and red) vegetables each day
- Have water by your bed each night
- As soon as you get up in the morning drink a glass of water before you do anything else
- Drink (nonalcoholic) drinks with every meal
- Have at least two alcohol free days a week (and not two days where the drinks are free)
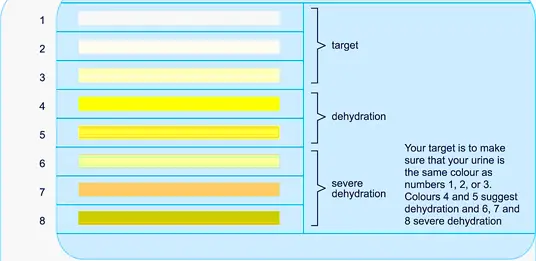
Use urine color to gauge your level of dehydration
Efficacy: Numerous studies have shown decreased performance in various states dehydration. They have also shown less strength in such individuals.
Side Effects: Over-hydration may cause hyponatremia (abnormally low level of sodium in blood serum: there may enough salt, but the concentration of salt ions is too diluted to do its job correctly). However, the amount of dehydration that causes hyponatremia (signs and symptoms may include nausea and vomiting, headache, confusion, loss of energy, fatigue, restlessness and irritability, muscle weakness, spasms or cramps, seizures, unconsciousness, coma) is usually quite excessive. It occurs over long periods (e.g., endurance or ultra-endurance events over four hours in length; for the rest of us, hyponatremia requires a daily lack of enough water for a long period or a fever of lesser duration). In chronic hyponatremia, sodium levels drop gradually over days or weeks — and symptoms and complications are typically more moderate.
In acute hyponatremia, sodium levels drop rapidly — resulting in potentially dangerous effects, such as rapid brain swelling, which can result in coma and death.
Premenopausal women appear to be at the greatest risk of hyponatremia-related brain damage. This may be related to the effect of women’s sex hormones on the body’s ability to balance sodium levels.
Gastrointestinal (GI) upset may occur, especially with fructose containing (fructose is a simple sugar found in honey and in many ripe fruits) fluid replacement drinks.
Dosage:

Daily water requirements by weight – athletes will require more
Timing water consumption
The American College of Sports Medicine suggests consumption of 400-600 mL of water two hours before exercise and 150 mL every 15-20 minutes of exercise. More is required in climates and/or temperatures with high perspiration rates. They further recommended the addition of carbohydrates for activities greater than 90 minutes (sports drink have this component). Hydration after exercise is also very important.
Considering the very high quality of training and conditioning personnel at Oregon, I am certain that the guidelines discussed here are refined and individualized for each Duck athlete, and that they are administered and managed at the very highest professional standards.
These articles are designed to provide information about supplementation so that the reader understands what the state of legal supplementation is like. For those of us weekend warriors or other athletes not connected to the elite training that Duck athletes receive, this article, and others like it in the past and to come, will educate us as to how best to keep our bodies healthy and prepared for exercise and sports.
This ends the discussion for today. The next article (Part 3b) will include several more supplements commonly used by athletes.
Congratulations to ALL the Oregon teams for their great achievements this year!
Up Next: Coach Helfrich and the Ducks prepare for another exciting and successful season in 2013-2014.
GO DUCKS!
Top Photo by Eugene Johnson
Related Articles:
NeuroDocDuck (Dr. Driesen) is a doctor who specializes in neurology, and sports medicine. He is an Oregon alumnus, completing his medical education and training in the UK. He has been both a practicing clinician and professor, a well-known and respected diagnostician, an author, and has appeared on national television.
NeuroDocDuck is active in his profession, and stays current on all new trends in his field. He enjoys golf and loves his Ducks!