
Sports Medicine
All You Wanted to Know About Vitamins, Minerals, and Nutritional Supplements
In Part 4d of this series about Vitamins, Minerals, and Nutritional Supplements, we will explore dietary supplements used by all of us – athletes and nonathletes – for our health. It is an extension of Part 4b and will be the last article of this series.
We include a great deal of well-researched, up-to-date medical information about some of the supplements you may take, or are thinking of taking, so that you can use it to get the most out of them while using them safely.
|
‘Buyer Beware’ Information about Supplementation |
Most supplements are not tested adequately for efficacy, purity, or safety. |
Be careful of misleading product information. |
‘Natural’ does not mean safe! |
‘More’ is seldom better! |
Nothing replaces a well-balanced diet that includes a variety of high-quality foods with plenty of nutrients. |
Athletes, and others, use supplements at their own risk! |
Gingko Biloba:
Claims: There are many uses associated with gingko biloba: to improve cognitive function in dementia, including Alzheimer’s disease: to treat vascular insufficiency (central and peripheral), dysmenorrhea, and acute mountain sickness; and to improve sleep in depression patients.
Mechanism: Gingko biloba is a free radical scavenger and inhibitor of monoamine oxidase (found in the outer membrane of mitochondria that degrade biogenic amines and are thus responsible for the destruction of transmitter substances at neuronal synapses). MAO inhibitors are often used in clinical depression to block such destruction.
Efficacy: According to the Mayo Clinic, the most promising clinical results right now are in the areas of claudication symptoms (leg pain which results from clogged arteries) and multi-infarct dementia (localized necrosis resulting from obstruction of the blood supply and early-stage Alzheimer’s disease leads to dementia).
Good results have been seen for dietary supplementation of gingko biloba and what is being called “cerebral insufficiency,” which includes poor concentration, absentmindedness, confusion, decreased physical performance, fatigue, headache, dizziness, depression, and anxiety.
According to studies done for the U.S. military by the National Academy of Sciences, this dietary supplement does pretty well. However, there are a few concerns of which to be aware. Their review shows that in younger and healthy subjects, high acute dosing may enhance mental performance for short periods. Longer dosing for the same purpose still requires additional research.
The report also discussed benefits that may be seen in the treatment of cardiovascular disease by reducing nanoplaque formation in high-risk cardiovascular patients. There are also benefits to liver function as reported through animal models because of the anti-inflammatory and antioxidant properties.
Side Effects:
Side effects of ginkgo biloba may include headache, nausea, gastrointestinal upset, diarrhea, dizziness, or allergic skin reactions. More severe allergic reactions have occasionally been reported.
There are some data to suggest that ginkgo biloba can increase bleeding risk, so people who take anticoagulant drugs, have bleeding disorders, or have scheduled surgery or dental procedures should use caution, and talk to a health care provider if using ginkgo.
Fresh (raw) ginkgo seeds contain large amounts of a chemical called ginkgotoxin, which can cause serious adverse reactions—even seizures and death. Roasted seeds can also be dangerous. Products made from standardized ginkgo leaf extracts contain little ginkgotoxin and appear to be safe when used orally and appropriately. Stay away from gingko biloba seeds!
Tell all your health care providers about any complementary health practices you use. Give them a full picture of what you do to manage your health. This will help ensure coordinated and safe care. For tips about talking with your health care providers about complementary and alternative medicine, see NCCAM’s Time to Talk campaign.
Dosage: Traditional recommendations include ginkgo products containing 24% flavoglycosides (also called flavone glycosides or flavones) and 6% terpenes: 80-240 milligrams of a 50:1 standardized leaf extract daily, or 3-6 milliliters of a 40 milligram per milliliter liquid extract in 2-3 divided doses, or 30-40 milligrams of extract in a tea bag, prepared as a tea, for at least 4-6 weeks. There is a lack of evidence in support of the clinical benefit of small concentrations of ginkgo found in fortified foods. All doses above are oral unless otherwise stated. Beneficial effects may take 4-6 weeks to appear. Ginkgo seeds are potentially toxic and should be avoided. The intravenous ginkgo product Tebonin®, which was available in Germany, was removed from the German market due to significant adverse effects.
40-240 milligrams of extract, tincture, or powder has been taken by mouth daily, divided into two or three doses. Beneficial effects may take 4-6 weeks to appear. Patients have also been treated with intravenous ginkgo preparations: 0.7mg of intravenous extract per minute for 120 minutes, or 100 mg of ginkgo in 500 cubic centimeters of normal saline, administered twice daily. Also, 20 milliliters of ginkgo in 250 milliliters of normal saline daily for four weeks and 200 milligrams of EGb 761 infusion for 10 days, followed by a twice-daily oral dose of 80 milligrams for 12 weeks.
The effects of EGb 761 on the central nervous system (CNS) underlie one of its major therapeutic indications; (i.e., individuals suffering from deteriorating cerebral mechanisms related to age-associated impairments of memory, attention and other cognitive functions).
EGb 761 is currently used as symptomatic treatment for cerebral insufficiency that occurs during normal ageing or which may be due to degenerative dementia, vascular dementia (caused by blood vessel problems) or mixed forms of both, and for neurosensory disturbances. Depressive symptoms of patients with Alzheimer’s disease (AD) and aged non-Alzheimer patients may also respond to treatment with EGb 761 since this extract has an “anti-stress” effect.
Basic and clinical studies, conducted both in vitro and in vivo, support these beneficial neuroprotective effects of EGb 761. EGb 761 has several major actions; it enhances cognition, improves blood rheology (the branch of physics that studies the deformation and flow of matter and tissue metabolism, and opposes the detrimental effects of ischæmia).
Several mechanisms of action are useful in explaining how EGb 761 benefits patients with AD and other age-related, neurodegenerative disorders. In animals, EGb 761 possesses antioxidant and free radical-scavenging activities. It reverses age-related losses in brain alpha 1-adrenergic, 5-HT1A and muscarinic receptors, protects against ischæmic neuronal death (In medicine, ischæmia is a restriction in blood supply to tissues, causing a shortage of oxygen and glucose needed for cellular metabolism. Ischæmia is generally caused by problems with blood vessels, with resultant damage to or dysfunction of tissue. It also means local anemia in a given part of a body sometimes resulting from congestion, preserves the function of the hippocampal mossy fiber system (memory processing), increases hippocampal high-affinity choline uptake, inhibits the down-regulation of hippocampal glucocorticoid receptors, enhances neuronal plasticity, and counteracts the cognitive deficits that follow stress or traumatic brain injury (this includes MTBI, a possible problem with concussions). Identified chemical constituents of EGb 761 have been associated with certain actions. Both flavonoid and ginkgolide constituents are involved in the free radical-scavenging and antioxidant effects of EGb 761, which decrease tissue levels of reactive oxygen species (ROS) and inhibit membrane lipid peroxidation.
Regarding EGb 761-induced regulation of cerebral glucose utilization, bilobalide increases the respiratory control ratio of mitochondria by protecting against uncoupling of oxidative phosphorylation, thereby increasing ATP levels (high-energy molecule that stores the energy we need to do just about everything we do). It is present in the cytoplasm and nucleoplasm of every cell, and essentially all the physiological mechanisms that require energy for operation obtain it directly from the stored ATP.
With regard to its “anti-stress” effect, EGb 761 acts to decrease the expression of the peripheral benzodiazepine receptor (PBR) of the adrenal cortex. The peripheral-type benzodiazepine receptor was identified in peripheral tissues because of its ability to bind the benzodiazepine diazepam (Valium™). Peripheral-type receptors for diazepam are those tissues outside of the central nervous system (brain and spine).
PBRs seem to be involved in the regulation of several major stress systems: the HPA axis (hypothalamic-pituitary-adrenal stress system), the sympathetic nervous system, the renin-angiotensin axis, and the neuroendocrine-immune axis.
In a human study, platelet PBRs were assessed in psychiatric residents (young doctors) who were completing the written part of the Israeli board-certification examination in comparison with age- and sex-matched controls. The platelet PBR density was significantly elevated immediately after the examination and showed a trend toward a decrease to normal range 10 days later. Similar changes were detected in anxiety levels, as measured by the appropriate rating scale (Karp et al., 1989). Thus, as shown in animal studies, acute stress in humans can lead to an increase in PBRs. Reducing PBR density is an anti-stress and anti-anxiety action.
Soy Isoflavonoids: They occur mainly in legumes with the highest concentrations in soybeans. Soybeans can be processed into soy protein, which is a powder; soy milk, which is a beverage that may or may not be fortified with extra calcium from the soybeans; or soy fiber, which contains some of the fibrous parts of the bean.
Claims: Soy isoflavonoids are used for menopausal symptoms and to prevent osteoporosis and heart disease in postmenopausal women. They are also used for hypertension and hyperlipidemia (hyper = beyond normal levels).
Mechanism: Isoflavones are hydrolyzed (decomposition of a compound by chemical reaction with water). By enzymes in the jejunum (central section of three of the small intestine) to phytoestrogens, which may then stimulate estrogen receptors in the heart, vasculature, bone, and bladder.
Estrogen, while usually thought of a female hormone, has an important role in men. As teenagers, men have high levels of testosterone and low levels of estrogen. As they age, testosterone levels in men decrease while their estrogen levels increase. Not surprisingly, high levels of estrogen in men usually correspond to low levels of testosterone. High estrogen levels in men contribute to prostate cancer and heart disease as well as gynecomastia (enlarged breasts). As the testosterone is transformed into estrogen, the low levels of testosterone can cause many unpleasant symptoms including loss of muscle mass, fatigue, low libido, erectile dysfunction, and small testes. Furthermore, excessive estrogen in men raises body fat and can contribute to diabetes and high lipids.
Testosterone will begin to convert to estrogen in men as they age due to the aromatase reaction. Aromatase is found most prevalently in fat cells, so the more body fat a man has, especially in the midsection, the more aromatase and hence the more estrogen. Your physician will order comprehensive blood spot testing which will measure your testosterone and estrogen levels (among others). The tests will inform your physician if your diminished testosterone is a result of the aromatase reaction. High estrogen in men can be corrected.
Efficacy: On the basis of the data presented, a study concluded that the evidence provided was insufficient to establish a cause and effect relationship between the consumption of soy isoflavones and reduction of vasomotor symptoms associated with menopause. Soy can reduce cholesterol when used in combination with a low-fat diet. In women near or after menopause, soy seems to be able to relieve hot flashes, reduce the risk of osteoporosis (weak bones), and possibly lower blood pressure.
In men, there is some evidence that soy milk might reduce the risk of developing prostate cancer.
Possibly Effective for:
| High cholesterol | Reducing the duration of diarrhea in infants |
| Hot flashes caused by menopause. But it doesn’t seem to help for hot flashes in women with breast cancer | Preventing and treating diabetic peripheral nerve problems |
| Reducing the risk of osteoporosis (weak bones) | Providing nutrition to infants who can’t digest milk sugars |
| Reducing the risk of developing breast cancer | Reducing protein in the urine of people with kidney disease |
| Treating diabetes type 2 |
Table 1. Possibly effective for these conditions.
Possibly Ineffective for: reducing muscle soreness caused by exercise and heart disease.
Insufficient Evidence to Rate Effectiveness for:
| preventing thyroid cancer | reducing breast pain |
| endometrial cancer | weight loss |
| lung cancer | asthma |
| prostate cancer | high blood pressure |
| improving memory | premenstrual syndrome (PMS); and other conditions |
Table 2. Insufficient evidence to rate effectiveness for these conditions.
Side Effects: Consuming soy foods such as soy protein is safe. Taking soy dietary supplements also seems to be safe for most people when used short-term. It can cause some mild side effects such as constipation, bloating, and nausea. It can also cause allergic reactions involving rash and itching in some people. Long-term use of high doses of soy dietary supplements might not be safe. Also, there is concern that taking high doses might cause abnormal tissue growth in the uterus.
Do not take soy in amounts greater than what is normally found in foods if you are or have: pregnant or breast-feeding; breast cancer, or if breast cancer runs in your family; endometrial cancer; kidney disease; and a risk of urinary bladder cancer.
Do not use soy in children without medical supervision.
For humans, the potency of soy isoflavones has raised concerns regarding the possibility that phytoestrogens may be a double-edged sword. On the one-hand, phytoestrogens may offer benefits to some groups, while perhaps creating risks to others. Speculation that isoflavones cause thyroid disease has been based on studies showing that genistein is capable of inhibiting thyroid peroxidase (TPO), a key enzyme in the production of thyroid hormones. These in vitro (outside the living organism) studies show that the potency of genistein is similar to that for a number of flavonoids that were also tested, and the latter group of phytoprotectants are found in abundance in fruits and vegetables. Indeed, dietary intake of flavonoids is estimated to be similar to that of isoflavones when soy foods are consumed. The IC50 value (the value is that concentration of a drug that reduces the activity, or binding, of another drug to an enzyme by 50%) for inhibition of TPO by daidzein and genistein was reported as 2.0 and 8.8 μM, respectively, and this is several orders of magnitude higher than the circulating plasma concentrations of free daidzein (approx. 10 nM and genistein (approx. 18 nM when usual dietary intakes of isoflavones are consumed). Thyroid hormone plays a key role in development and many studies have compared growth and development of infants fed soy formulas with those breast-fed: no significant differences were observed, although older soy formulas were not optimally formulated and did compromise development and growth. It is difficult to find case reports of adverse effects, either short-term or long-term, due to soy infant formula use. A recent study of a cohort of 952 adults who had been fed either soy formula or cow-milk formula as infants found no significant differences between the groups, either males or females, with regard to height, weight, BMI, indices of pubertal maturation and numerous other reproductive outcomes, including infertility, and cancer.
The real potential of soy foods containing isoflavones is most likely to be in the prevention of heart disease rather than in its treatment, as implied by the wording of the health claim. Amounts considerably less than the recommended 25 g/day soy protein are likely to be helpful in this regard. Soy protein intake by Japanese adults averages about 6-8 g/day and it was found that serum cholesterol levels in adults are inversely correlated with soy protein intake. Although several studies have failed to demonstrate any cholesterol-lowering effects of isoflavones when administered as supplements, their non-hormonal properties may be of greater significance in reducing risk for heart disease. Several clinical studies have shown that isoflavones reduce the susceptibility of lipids to oxidation, and they have been recently found to have digitalis-like effects in relaxing coronary arteries by a mechanism that involves antagonism of calcium channels. The anti-inflammatory properties of isoflavones in epithelial cells (membranous tissue composed of one or more layers of cells which forms the covering of most internal and external surfaces of the body and its organs internally, including the lining of vessels and other small cavities, and externally being the skin may also be important in protecting blood vessels).
Dosage:
For high cholesterol: 20-50 grams per day of soy protein.
For preventing weak bones (osteoporosis): 40 grams per day soy protein containing 2-2.25 mg isoflavones per gram.
For menopausal symptoms such as hot flashes: 20-60 grams per day of soy protein providing 34-76 mg isoflavones. Concentrated soy isoflavone extracts providing 50-120 mg/day of isoflavones.
Genistein, a soy isoflavone: 54 mg per day.
For protein in the urine of people with kidney disease: a diet limited to 700-800 mg/kg soy protein daily has been used.
For diarrhea in infants: soy fiber fortified formula containing 18-20 grams of soy protein per liter.
For type 2 diabetes: touchi extract 300 mg three times daily. Touchi (a fermented soy product made from black beans) is a traditional Chinese food prepared from soybeans.
For type 2 diabetes in postmenopausal women: 30 grams of soy protein daily, containing 132 mg of phytoestrogens daily for up to 12 weeks.
Soy foods contain variable amounts of isoflavones. Soy flour contains 2.6 mg isoflavones per gram of soy flour, fermented soybeans contain 1.3 mg per gram, boiled soybeans contain 0.6 mg per gram, soymilk contains 0.4 mg per gram, soybean curd contains 0.5 mg per gram, fried soybean curd contains 0.7 mg per gram, soybean paste contains 0.4 mg per gram, and soy sauce contains 0.016 mg per gram.
Vitamin C: Vitamin C, also known as L-ascorbic acid, is a water-soluble vitamin that is naturally present in some foods, added to others, and available as a dietary supplement. Humans, unlike most animals, are unable to synthesize vitamin C endogenously, so it is an essential dietary component
Claims: Vitamin C is said to prevent or reduce the duration of upper respiratory infections. Antioxidant properties are claimed to prevent cardiovascular disease and cancer. Vitamin C is used to treat hypertension, exercise-induced asthma, and osteoporosis. Claims also include that it speeds recovery from injury and improves absorption of iron from the GI tract (for anemia).
Mechanism: Vitamin C is required for the biosynthesis of collagen, L-carnitine, and certain neurotransmitters; vitamin C is also involved in protein metabolism. Collagen is an essential component of connective tissue, which plays a vital role in wound healing. Vitamin C is also an important physiological antioxidant and has been shown to regenerate other antioxidants within the body, including alpha-tocopherol (vitamin E). Ongoing research is examining whether vitamin C, by limiting the damaging effects of free radicals through its antioxidant activity, might help prevent or delay the development of certain cancers, cardiovascular disease, and other diseases in which oxidative stress plays a causal role. In addition to its biosynthetic and antioxidant functions, vitamin C plays an important role in immune function and improves the absorption of nonheme iron, the form of iron present in plant-based foods. Insufficient vitamin C intake causes scurvy, which is characterized by fatigue or lassitude, widespread connective tissue weakness, and capillary fragility.
Oral vitamin C produces tissue and plasma concentrations that the body tightly controls. Approximately 70%-90% of vitamin C is absorbed at moderate intakes of 30-180 mg/day. However, at doses above 1 g/day, absorption falls to less than 50% and absorbed, unmetabolized ascorbic acid is excreted in the urine. Results from pharmacokinetic studies indicate that oral doses of 1.25 g/day ascorbic acid produce mean peak plasma vitamin C concentrations of 135 micromol/L (a concentration of one-thousandths of a mole/liter – a mole is a molecular weight of a substance in grams), which are about two times higher than those produced by consuming 200-300 mg/day ascorbic acid from vitamin C-rich foods. Pharmacokinetic modeling predicts that even doses as high as 3 g ascorbic acid taken every 4 hours would produce peak plasma concentrations of only 220 micromol/L.
The total body content of vitamin C ranges from 300 mg (at near scurvy) to about 2 g. High levels of vitamin C (millimolar concentrations) are maintained in cells and tissues, and are highest in leukocytes (white blood cells), eyes, adrenal glands, pituitary gland, and brain. Relatively low levels of vitamin C (micromolar concentrations) are found in extracellular fluids, such as plasma, red blood cells, and saliva.
Efficacy: Cancer prevention and treatment: People with high intakes of vitamin C from fruits and vegetables might have a lower risk of getting many types of cancer, such as lung, breast, and colon cancer. However, taking vitamin C supplements, with or without other antioxidants, doesn’t seem to protect people from getting cancer.
It is not clear whether taking high doses of vitamin C is helpful as a treatment for cancer. Vitamin C’s effects appear to depend on how it is administered to the patient. Oral doses of vitamin C cannot raise blood levels of vitamin C nearly as high as intravenous doses given through injections. A few studies in animals and test tubes indicate that very high blood levels of vitamin C might shrink tumors. But more research is needed to determine whether high-dose intravenous vitamin C helps treat cancer in people.
Vitamin C dietary supplements and other antioxidants might interact with chemotherapy and radiation therapy for cancer. People being treated for cancer should talk with their oncologist before taking vitamin C or other antioxidant supplements, especially in high doses.
Cardiovascular disease: People who eat lots of fruits and vegetables seem to have a lower risk of cardiovascular disease. Researchers believe that the antioxidant content of these foods might be partly responsible for this association because oxidative damage is a major cause of cardiovascular disease. However, scientists aren’t sure whether vitamin C itself, either from food or supplements, helps protect people from cardiovascular disease. It is also not clear whether vitamin C helps prevent cardiovascular disease from getting worse in people who already have it.
Age-related macular degeneration (AMD) and cataracts: AMD and cataracts are two of the leading causes of vision loss in older people. Researchers do not believe that vitamin C and other antioxidants affect the risk of getting AMD. However, research suggests that vitamin C combined with other nutrients might help keep early AMD from worsening into advanced AMD.
In a large study, older people with AMD who took a daily dietary supplement with 500 mg vitamin C, 80 mg zinc, 400 IU vitamin E, 15 mg beta-carotene, and 2 mg copper for about 6 years had a lower chance of developing advanced AMD. They also had less vision loss than those who did not take the dietary supplement. More research is needed before doctors can recommend dietary supplements containing vitamin C for patients with AMD. However, people who have or are developing the disease might want to talk with their doctor about taking dietary supplements.
The relationship between vitamin C and cataract formation is unclear. Some studies show that people who get more vitamin C from foods have a lower risk of getting cataracts. But further research is needed to clarify this association and to determine whether vitamin C supplements affect the risk of getting cataracts.
The common cold: Although vitamin C has long been a popular remedy for the common cold, research shows that for most people, vitamin C supplements do not reduce the risk of getting the common cold. However, people who take vitamin C supplements regularly might have slightly shorter colds or somewhat milder symptoms when they do have a cold. Using vitamin C supplements after cold symptoms start does not appear to be helpful.
Taking too much vitamin C can cause diarrhea, nausea, and stomach cramps. In people with a condition called hemochromatosis, which causes the body to store too much iron, high doses of vitamin C could worsen iron overload and damage body tissues.
Acute vitamin C deficiency leads to scurvy. The timeline for the development of scurvy varies, depending on vitamin C body stores, but signs can appear within 1 month of little or no vitamin C intake (below 10 mg/day). Initial symptoms can include fatigue (probably the result of impaired carnitine biosynthesis), malaise, and inflammation of the gums. As vitamin C deficiency progresses, collagen synthesis becomes impaired and connective tissues become weakened, causing petechiae (pinpoint, round spots that appear on the skin as a result of bleeding under the skin. The bleeding causes the petechiae to appear red, brown, or purple, etc.). Additional signs of scurvy include depression as well as swollen, bleeding gums and loosening or loss of teeth due to tissue and capillary fragility. Iron deficiency anemia can also occur due to increased bleeding and decreased nonheme iron absorption secondary to low vitamin C intake. In children, bone disease can be present. Left untreated, scurvy is fatal.
Side Effects:
Vitamin C has low toxicity and is not believed to cause severe adverse effects at high intakes. The most common complaints are diarrhea, nausea, abdominal cramps, and other gastrointestinal disturbances due to the osmotic effect of unabsorbed vitamin C in the gastrointestinal tract.
Hyperoxaluria (excess oxalic acid or oxalates in the urine), hematuria (blood in the urine), crystalluria (presence of crystals in the urine), hyperuricosuria (excessive amounts of uric acid in the urine), and predisposition to kidney stone formation may be related to greater than 1 gram/day of Vitamin C. High vitamin C intakes also have the potential to increase urinary oxalate and uric acid excretion, which could contribute to the formation of kidney stones, especially in individuals with renal disorders. However, studies evaluating the effects on urinary oxalate excretion of vitamin C intakes ranging from 30 mg to 10 g/day have had conflicting results, so it is not clear whether vitamin C actually plays a role in the development of kidney stones. The best evidence is that vitamin C contributes to kidney stone formation in patients with pre-existing hyperoxaluria (see first paragraph of this section for definition).
Under certain conditions, vitamin C can act as a pro-oxidant, potentially contributing to oxidative damage. A few studies in vitro (outside the living body) have suggested that by acting as a pro-oxidant, supplemental oral vitamin C could cause chromosomal and/or DNA damage and possibly contribute to the development of cancer. However, other studies have not shown increased oxidative damage or increased cancer risk with high intakes of vitamin C.
Other reported effects of high intakes of vitamin C include reduced vitamin B12 and copper levels, accelerated metabolism or excretion of ascorbic acid, erosion of dental enamel, and allergic responses. However, at least some of these conclusions were a consequence of assay artifact, and additional studies have not confirmed these observations.
Vitamin C dietary supplements might interact with cancer treatments, such as chemotherapy and radiation therapy. It is not clear whether vitamin C might have the unwanted effect of protecting tumor cells from cancer treatments or whether it might help protect normal tissues from getting damaged. If you are being treated for cancer, check with your health care provider before taking vitamin C or other antioxidant supplements, especially in high doses.
In one study, vitamin C plus other antioxidants (such as vitamin E, selenium, and beta-carotene) reduced the heart-protective effects of two drugs taken in combination (a statin and niacin) to control blood-cholesterol levels. It is not known whether this interaction also occurs with other statins. Health care providers should monitor lipid levels in people taking both statins and antioxidant supplements.
In people with a condition called hemochromatosis, which causes the body to store too much iron taking too much vitamin C, could worsen iron overload and damage body tissues.
The message here is that while megadoses of vitamin C may be helpful in some cases, it is best to avoid large doses beyond 1 g/day. For most people, the guidelines below should be the most beneficial.
Tell your doctor about any dietary supplements and medicines you take. They can tell you if those dietary supplements might interact or interfere with your prescription or over-the-counter medicines or if the medicines might interfere with how your body absorbs, uses, or breaks down nutrients.
Dosage:
Recommended daily allowance (RDA): * Adequate Intake (AI)
|
Age |
Male |
Female |
Pregnancy |
Lactation |
|
| 0-6 months |
40 mg* |
40 mg* |
|
|
|
| 7-12 months |
50 mg* |
50 mg* |
|
|
|
| 1-3 years |
15 mg |
15 mg |
|
|
|
| 4-8 years |
25 mg |
25 mg |
|
|
|
| 9-13 years |
45 mg |
45 mg |
|
|
|
| 14-18 years |
75 mg |
65 mg |
80 mg |
115 mg |
|
| 19+ years |
90 mg |
75 mg |
85 mg |
120 mg |
|
| Smokers | Individuals who smoke require 35 mg/day more vitamin C than nonsmokers. |
||||
Table 3. RDAs for Vitamin C.
|
Age |
Male |
Female |
Pregnancy |
Lactation |
| 0-12 months |
Not possible to establish* |
Not possible to establish* |
|
|
| 1-3 years |
400 mg |
400 mg |
|
|
| 4-8 years |
650 mg |
650 mg |
|
|
| 9-13 years |
1,200 mg |
1,200 mg |
|
|
| 14-18 years |
1,800 mg |
1,800 mg |
1,800 mg |
1,800 mg |
| 19+ years |
2,000 mg |
2,000 mg |
2,000 mg |
2,000 mg |
Tolerable Upper Safe Limit for Vitamin C:
*Formula and food should be the only sources of vitamin C for infants.
Table 4. Tolerable upper safe limits for Vitamin C.
Vitamin D: Vitamin D is both a nutrient we eat and a hormone our bodies make. Few foods are naturally rich in vitamin D, so the biggest dietary sources of vitamin D are fortified foods and vitamin supplements. Good sources include dairy products and breakfast cereals (both of which are fortified with vitamin D), and fatty fish such as salmon and tuna.
For most people, the best way to get enough vitamin D is by taking a supplement, but the level in most multivitamins (400 IU) is too low. Encouragingly, some manufacturers have begun adding 800 or 1,000 IU of vitamin D to their standard multivitamin preparations. If the multivitamin you take does not have 1,000 IU of vitamin D, you may want to consider adding a separate vitamin D supplement, especially if you don’t spend much time in the sun. Talk to your doctor.
Two forms of vitamin D are used in supplements: vitamin D2 (“ergocalciferol,” or pre-vitamin D) and vitamin D3 (“cholecalciferol”). Vitamin D3 is chemically indistinguishable from the form of vitamin D produced in the body.
The body also manufactures vitamin D from cholesterol, through a process triggered by the action of sunlight on skin, hence its nickname, “the sunshine vitamin.” Yet some people do not make enough vitamin D from the sun, among them, people who have a darker skin tone, who are overweight, who are older, and who cover up when they are in the sun.
Correctly applied sunscreen reduces our ability to absorb vitamin D by more than 90 percent. And, not all sunlight is created equal: The sun’s ultraviolet B (UVB) rays—the so-called “tanning” rays, and the rays that trigger the skin to produce vitamin D—are stronger near the equator and weaker at higher latitudes. So in the fall and winter, people who live at higher latitudes (in the northern U.S. and Europe, for example) can’t make much if any vitamin D from the sun.
Claims: Vitamin D helps ensure that the body absorbs and retains calcium and phosphorus, both critical for building bone. Laboratory studies show that vitamin D can reduce cancer cell growth and plays a critical role in controlling infections. Many of the body’s organs and tissues have receptors for vitamin D, and scientists are still teasing out its other possible functions.
Several promising areas of vitamin D research look far beyond vitamin D’s role in building bones. And, as you might expect, the news media release a flurry of reports every time another study links vitamin D to some new ailment. These reports can be confusing, however, because some studies are stronger than others, and any report needs to be interpreted in the light of all other evidence. More answers may come from randomized trials, such as the Vitamin D and OmegA-3 Trial (VITAL), which will enroll 20,000 healthy men and women to see if taking 2,000 IU (International Unit is a unit of measurement for the amount of a substance, based on biological activity or effect).
Several studies link low vitamin D levels with an increased risk of fractures in older adults, and they suggest that vitamin D supplementation may prevent such fractures—as long as it is taken in a high enough dose.
A summary of the evidence comes from a combined analysis of 12 fracture prevention trials that included more than 40,000 elderly people, most of them women. Researchers found that high intakes of vitamin D supplements—of about 800 IU per day—reduced hip and non-spine fractures by 20 percent, while lower intakes (400 IU or less) failed to offer any fracture prevention benefit. IU Several studies link low vitamin D levels with an increased risk of fractures in older adults, and they suggest that vitamin D supplementation may prevent such fractures—as long as it is taken in a high enough dose.
Vitamin D may also help increase muscle strength, which in turn helps to prevent falls, a common problem that leads to substantial disability and death in older people. Once again, vitamin D dose matters: A combined analysis of multiple studies found that taking 700 to 1,000 IU of vitamin D per day lowered the risk of falls by 19 percent, but taking 200 to 600 IU per day did not offer any such protection.
A recent vitamin D trial drew headlines for its unexpected finding that a very high dose of vitamin D increased fracture and fall risk in older women. The trial’s vitamin D dose—500,000 IU taken in a once-a-year pill—was much higher than previously tested in an annual regimen. After up to 5 years of treatment, women in the vitamin D group had a 15 percent higher fall risk and a 26 percent higher fracture risk than women who received the placebo.
It’s possible that giving the vitamin D in one large dose, rather than in several doses spread throughout the year, led to the increased risk. The study authors note that only one other study—also a high-dose, once-a-year regimen—found vitamin D to increase fracture risk; no other studies have found vitamin D to increase the risk of falls. Furthermore, there’s strong evidence that more moderate doses of vitamin D taken daily or weekly protect against fractures and falls—and are safe.
So what is the significance of this study for people who want to take vitamin D supplements? A reasonable conclusion would be to continue taking moderate doses of vitamin D3 regularly, since these have a strong safety record, but to avoid extremely high single doses. This recent finding does present a challenge to scientists who will work to understand why the extreme single dose appears to have adverse effects.
Vitamin D may also help increase muscle strength, which in turn helps to prevent falls, a common problem that leads to substantial disability and death in older people. Once again, vitamin D dose matters: A combined analysis of multiple studies found that taking 700 to 1,000 IU of vitamin D per day lowered the risk of falls by 19 percent, but taking 200 to 600 IU per day did not offer any such protection. [I have osteoporosis and take 5000 mg/day D3 along with 1000 mg/day of calcium – the amount to be used should be determined by your doctor and should take into consideration such factors as age, health status, genetics, disorders, medications, and supplements taken.]
Mechanism: The active form of vitamin D (D3) binds to intracellular receptors (internal cell receptors) that then function as transcription factors (synthesis of RNA from a DNA template to modulate gene expression). This process is an ongoing one that occurs many times/second, 24 hours/day.
Part of the roles DNA and RNA play within the nucleus of cells is to produce proteins that are involved in the regulation of the body and behavior. Vitamin D, as a hormone, makes it possible to alter gene expression to meet new internal or environmental events. Thus, vitamin D assists in adaptation to new events or problems.
Some primary transcripts are never translated into protein. These RNA molecules have other functions in the cell.
The active hormonal form of vitamin D (D3), has a central role in calcium and phosphate homeostasis and the maintenance of bone. Apart from its calcitropic effects (any material (especially a hormone) that is involved in the regulation of calcium in the blood and in bone). D3 regulates cell growth and differentiation in many target tissues. The effects of D3 are mediated by the vitamin D receptor (VDR), a member of the nuclear receptor superfamily of transcriptional regulators that also includes steroid, thyroid, retinoid, and many orphan receptors. Upon binding the hormone, the VDR regulates gene expression by direct interaction with specific sequence elements in the promoter region (a promoter is a sequence of DNA needed to turn a gene on or off). The process of transcription is initiated at the promoter. Usually found near the beginning of a gene, the promoter has a binding site for the enzyme used to make a messenger RNA (mRNA) molecule of hormone-responsive target genes. Vitamin D3 has physiologic effects much broader that a role in mineral homeostasis and bone function. This is an active area of research and a much better understanding of this area will likely be available in the near future.
Efficacy:
The effectiveness ratings for Vitamin D3 are as follows:
Effective for:
| Treating conditions that cause weak and painful bones (osteomalacia). | Low blood calcium levels because of a low parathyroid thyroid hormone levels. |
| Low levels of phosphate in the blood (familial hypophosphatemia). | Helping prevent low calcium and bone loss (renal osteodystrophy) in people with kidney failure. |
| Low levels of phosphate in the blood due to a disease called Fanconi syndrome. | Rickets. |
Psoriasis (with a specialized prescription-only form of vitamin D).Vitamin D deficiency.
Table 5. Effectiveness of Vitamin D3 supplementation in these conditions
Likely effective for:
Treating osteoporosis (weak bones). Taking cholecalciferol (vitamin D3) along with calcium seems to help prevent bone loss and bone breaks.
Preventing falls in older people. Researchers noticed that people who don’t have enough vitamin D tend to fall more often than other people. They found that taking a vitamin D supplement reduces the risk of falling by up to 22%. Higher doses of vitamin D are more effective than lower doses. One study found that taking 800 IU of vitamin D reduced the risk of falling, but lower doses didn’t.
Also, vitamin D, in combination with calcium, but not calcium alone, may prevent falls by decreasing body sway and blood pressure. This combination prevents more falls in women than men.
Reducing bone loss in people taking drugs called corticosteroids.
Possibly effective for:
Reducing the risk of multiple sclerosis (MS). Studies show taking vitamin D seems to reduce women’s risk of getting MS by up to 40%. Taking at least 400 IU per day, the amount typically found in a multivitamin supplement, seems to work the best.
Preventing cancer. Some research shows that people who take a high-dose vitamin D supplement plus calcium might have a lower chance of developing cancer of any type.
Weight loss. Women taking calcium plus vitamin D are more likely to lose weight and maintain their weight. But this benefit is mainly in women who didn’t get enough calcium before they started taking supplements.
Respiratory infections. Clinical research in school aged children shows that taking a vitamin D supplement during winter might reduce the chance of getting seasonal flu. Other research suggests that taking a vitamin D supplement might reduce the chance of an asthma attack triggered by a cold or other respiratory infection. Some additional research suggests that children with low levels of vitamin D have a higher chance of getting a respiratory infection such as the common cold or flu.
Reducing the risk of rheumatoid arthritis in older women.
Reducing bone loss in women with a condition called hyperparathyroidism.
Preventing tooth loss in the elderly.
Possibly ineffective for:
Breast cancer. Many studies have looked at whether vitamin D can help prevent breast cancer, but their results have not always agreed. The best evidence to date comes from a large study called the Women’s Health Initiative, which found that taking 400 IU of vitamin D and 1000 mg of calcium per day does not seem to lower the chance of getting breast cancer. The possibility remains that high doses of vitamin D might lower breast cancer risk in younger women. But the doses needed would be so high that they might not be safe.
High blood pressure.
Improving muscle strength in older adults.
Preventing bone loss in people with kidney transplants.
Insufficient evidence to rate effectiveness for:
Asthma. Some research suggests that people with asthma are more likely to have low vitamin D levels in the body. In children with asthma, taking a vitamin D supplement might reduce the chance of an asthma attack during a cold or other respiratory infection. But it is too soon to know if taking a vitamin D supplement can prevent or treat asthma symptoms.
Heart disease. Research suggests that people with low levels of vitamin D in their blood are much more likely to develop heart disease, including heart failure, than people with higher vitamin D levels. However, taking vitamin D does not seem to extend the life of people with heart failure.
Chronic obstructive pulmonary disease (COPD). Some research shows that people with COPD have lower than normal vitamin D levels. But there is not enough information to know if taking a vitamin D supplement can decrease symptoms of COPD.
High cholesterol. People with lower vitamin D levels seem to be much more likely to have high cholesterol than people with higher vitamin D levels. Limited research shows that taking calcium plus vitamin D daily, in combination with a low-calorie diet, significantly raises “good (HDL) cholesterol” and lowers “bad (LDL) cholesterol” in overweight women. But taking calcium plus vitamin D alone, does not reduce LDL cholesterol levels.
Gum disease. Higher blood levels of vitamin D seem to be linked with a reduced risk of gum disease in people 50 years of age or older. But, this doesn’t seem to be true for adults younger than 50.
Diabetes. People with lower vitamin D levels are significantly more likely to have type 2 diabetes compared to people with higher vitamin D levels. But, there is no reliable evidence that taking vitamin D supplements can treat or prevent type 2 diabetes. However, a proper level of D3 is useful for overall good health in diabetics if prescribedby a doctor.
Premenstrual syndrome (PMS). There is some evidence that getting more vitamin D from the diet might help to prevent PMS or reduce symptoms. Taking vitamin D supplements might help reduce symptoms but doesn’t seem to help prevent PMS.
A blood cell disease called myelodysplastic syndrome.
A muscle disease called proximal myopathy.
Colorectal cancer.
Warts.
Bronchitis.
Asthma.
Breathing disorders.
Metabolic syndrome.
Muscle pain caused by medications called “statins.”
Vaginal atrophy.
Other conditions: A promising report in the Archives of Internal Medicine suggests that taking vitamin D3 supplements may even reduce overall mortality rates: A combined analysis of multiple studies found that taking modest levels of vitamin D3 supplements was associated with a statistically significant 7 percent reduction in mortality from any cause. The analysis looked at the findings from 18 randomized controlled trials that enrolled a total of nearly 60,000 study participants; most of the study participants took between 400 and 800 IU of vitamin D3 per day for an average of five years. Keep in mind that this analysis has several limitations, chief among them the fact that the studies it included were not designed to explore mortality in general, or explore specific causes of death. More research is needed before any broad claims can be made about vitamin D and mortality.
More evidence is needed to rate vitamin D for these uses.
Side Effects:
Excessive exposure to sunlight does not lead to overproduction of vitamin D. Vitamin D toxicity is inevitably the result of overdosing on vitamin D supplements. Certainly, vitamin D3 supplements are a valuable treatment for individuals with deficiencies. However, ingestion of excessive (milligram) quantities of vitamin D3 over periods of weeks of months can be severely toxic to humans and animals. In fact, baits containing large quantities of vitamin D3 are used very effectively as rodenticides.
Vitamin D3 is likely safe when taken by mouth in recommended amounts. Most people do not commonly experience side effects with vitamin D3, unless too much is taken. Some side effects of taking too much vitamin D include weakness, fatigue, sleepiness, headache, loss of appetite, dry mouth, metallic taste, nausea, vomiting, and others.
Taking vitamin D3 for long periods of time in doses higher than >4000 units per day is possibly unsafe and may cause excessively high levels of calcium in the blood. However, much higher doses are often needed for the short-term treatment of vitamin D deficiency. This type of treatment should be done under the supervision of a doctor.
Special precautions & warnings:
| Pregnancy and breast-feeding: Vitamin D3 is likely safe during pregnancy and breast-feeding when used in daily amounts below 4000 units. Do not use higher doses. Using higher doses might cause serious harm to the infant. | Histoplasmosis: Vitamin D may increase calcium levels in people with histoplasmosis (an infection caused by breathing in spores of a fungus often found in bird and bat droppings. Histoplasmosis is most commonly transmitted when these spores become airborne, often during cleanup or demolition projects. This could lead to kidney stones and other problems. Use vitamin D cautiously. |
| Kidney disease: Vitamin D3 may increase calcium levels and increase the risk of “hardening of the arteries” in people with serious kidney disease. This must be balanced with the need to prevent renal osteodystrophy, a bone disease that occurs when the kidneys fail to maintain the proper levels of calcium and phosphorus in the blood. Calcium levels should be monitored carefully in people with kidney disease. | Over-active parathyroid gland (hyperparathyroidism): Vitamin D may increase calcium levels in people with hyperparathyroidism. Use vitamin D cautiously. |
| High levels of calcium in the blood: Taking vitamin D could make this condition worse. | Lymphoma: Vitamin D may increase calcium levels in people with lymphoma. |
| “Hardening of the arteries” (atherosclerosis): Taking vitamin D could make this condition worse. | This could lead to kidney stones and other problems. Use vitamin D cautiously. |
Sarcoidosis: Sarcoidosis is a disease of unknown cause that leads to inflammation. This disease affects body organs. Normally, the immune system defends the body against foreign or harmful substances. For example, it sends special cells to protect organs that are in danger. These cells release chemicals that recruit other cells to isolate and destroy the harmful substance. Inflammation occurs during this process. Once the harmful substance is gone, the cells and the inflammation go away.
In people who have sarcoidosis, the inflammation doesn’t go away. Instead, some of the immune system cells cluster to form lumps called granulomas in various organs in the body. Vitamin D may increase calcium levels in people with sarcoidosis. This could lead to kidney stones and other problems. Use vitamin D cautiously.
Table 6. Special precautions & warnings for Vitamin D supplementation.
Dosage. Efficacy for several health endpoints requires levels of 80 nmol/L or higher. Toxicity occurs at levels of 500 nmol/L or higher. The input needed for efficacy, in addition to typical food and cutaneous inputs, will usually be 1000-2000 IU/day of supplemental cholecalciferol (D3). Toxicity is associated only with excessive supplemental intake (usually well above 20,000 IU/day).
There is a difference between normal and optimal. Primitive man likely developed in tropical and sub-tropical conditions with large exposure to UV-B and its secondary consequence to skin exposure, vitamin D. Primitive environmental availability of a nutrient does not necessarily establish the higher requirements, but these exposures would have influenced the evolution of the relevant physiology, and such concentrations should at least be considered presumptively acceptable.
Some experts may disagree with the following ranges, but they are taken from healthy people in tropical or subtropical parts of the world, where they are receiving healthy sun exposures. It seems more than reasonable to assume that these values are in fact reflective of an optimal human requirement.
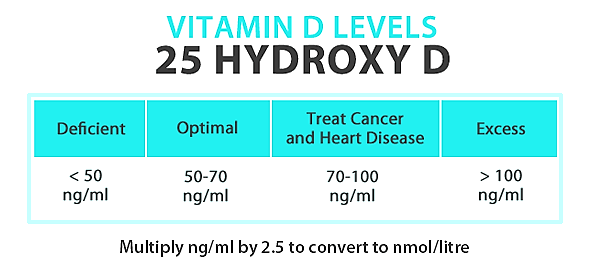
Figure 2. Desirable Vitamin D levels
Desirable Vitamin D Levels Under Four Conditions:
Vitamin E: Vitamin E is found naturally in some foods, added to others, and available as a dietary supplement. “Vitamin E” is the collective name for a group of fat-soluble compounds with distinctive antioxidant activities.
Naturally occurring vitamin E exists in eight chemical forms (alpha-, beta-, gamma-, and delta-tocopherol and alpha-, beta-, gamma-, and delta-tocotrienol) that have varying levels of biological activity. Alpha- (or α-) tocopherol is the only form that is recognized to meet human requirements.
Foods that contain vitamin E include eggs, fortified cereals, fruit, green leafy vegetables (such as spinach), meat, nuts, nut oils, poultry, vegetable oils (corn, cottonseed, safflower, soybean, sunflower, argan oil, olive oil, wheat germ oil), and whole grains. Cooking and storage may destroy some of the vitamin E in foods.
Claims:
Many claims have been made about vitamin E’s potential to promote health and prevent and treat disease. The mechanisms by which vitamin E might provide this protection include its function as an antioxidant and its roles in anti-inflammatory processes, inhibition of platelet aggregation, and immune enhancement.
Antioxidants (e.g., vitamin E) protect cells from the damaging effects of free radicals, which are molecules that contain an unshared electron. Free radicals damage cells and might contribute to the development of cardiovascular disease and cancer. Unshared electrons are highly energetic and react rapidly with oxygen to form reactive oxygen species (ROS). The body forms ROS endogenously when it converts food to energy, and antioxidants might protect cells from the damaging effects of ROS. The body is also exposed to free radicals from environmental exposures, such as cigarette smoke, air pollution, and ultraviolet radiation from the sun. ROS are part of signaling mechanisms among cells.
In addition to its activities as an antioxidant, vitamin E is involved in immune function and, as shown primarily by in vitro studies of cells, cell signaling, regulation of gene expression, and other metabolic processes. Alpha-tocopherol inhibits the activity of protein kinase C, an enzyme involved in cell proliferation and differentiation in smooth muscle cells, platelets, and monocytes. Vitamin-E-replete endothelial cells lining the interior surface of blood vessels are better able to resist blood-cell components adhering to this surface. Vitamin E also increases the expression of two enzymes that suppress arachidonic acid metabolism, thereby dilating blood vessels and inhibiting platelet aggregation.
Mechanism: Serum concentrations of vitamin E (alpha-tocopherol) depend on the liver, which takes up the nutrient after the various forms are absorbed from the small intestine. The liver preferentially re secretes only alpha-tocopherol via the hepatic (liver) alpha-tocopherol transfer protein. The liver metabolizes and excretes the other vitamin E forms. As a result, blood and cellular concentrations of other forms of vitamin E are lower than those of alpha-tocopherol and have been the subjects of less research.
Free radicals, such as superoxide, hydroxyl ions and nitric oxide all contain an unpaired electron. These radicals can have a negative effect on cells causing oxidative damage that leads to cell death. Antioxidants, such as vitamin E, prevent cell damage by binding to the free radical and neutralizing its unpaired electron. For example, when vitamin E binds to OO or O2 they form an intermediate structure that is converted to a-tocopherolquinone. A recent population based study of antioxidants concluded that a diet rich in foods containing vitamin E might help protect some people against Alzheimer’s disease (AD). Vitamin E in the form of supplements was not associated with a reduction in the risk of AD.
Efficacy: Evidence that vitamin E could help prevent or delay coronary heart disease (CHD) comes from several sources. In vitro studies have found that the nutrient inhibits oxidation of low-density lipoprotein (LDL) cholesterol, thought to be a crucial initiating step for atherosclerosis [6]. Vitamin E might also help prevent the formation of blood clots that could lead to a heart attack or venous thromboembolism.
In general, clinical trials have not provided evidence that routine use of vitamin E supplements prevents cardiovascular disease or reduces its morbidity and mortality. However, participants in these studies have been largely middle-aged or elderly individuals with demonstrated heart disease or risk factors for heart disease. Some researchers have suggested that understanding the potential utility of vitamin E in preventing CHD (coronary heart disease) might require longer studies in younger participants taking higher doses of the supplement. Further research is needed to determine whether supplemental vitamin E has any protective value for younger, healthier people at no obvious risk of CHD.
Antioxidant nutrients like vitamin E protect cell constituents from the damaging effects of free radicals that, if unchecked, might contribute to cancer development. Vitamin E might also block the formation of carcinogenic nitrosamines formed in the stomach from nitrites in foods and protect against cancer by enhancing immune function. Unfortunately, human trials and surveys that have attempted to associate vitamin E intake with cancer incidence have found that vitamin E is not beneficial in most cases.
Age-related macular degeneration (AMD) and cataracts are among the most common causes of significant vision loss in older people. Vitamin E could be used to prevent or treat these conditions. Overall, the available evidence is inconsistent with respect to whether vitamin E supplements, taken alone or in combination with other antioxidants, can reduce the risk of developing AMD or cataracts. However, the formulations of vitamin E, other antioxidants, zinc, and copper holds promise for slowing the progression of AMD in people with early-stage disease.
In summary, most research results do not support the use of vitamin E supplements by healthy or mildly impaired individuals (e.g., mild to low-moderate Alzheimer’s disease) to maintain cognitive performance or slow its decline with normal aging. More research is needed to identify the role of vitamin E, if any, in the management of cognitive impairment.
Side Effects: For short periods of time, vitamin E supplementation is generally considered safe at doses up to the recommended tolerable upper intake level (UL). However, vitamin E is possibly unsafe when used orally at doses exceeding the tolerable upper intake level. The recommended dietary allowance (RDA) obtained through food consumption is considered to be safe and beneficial.
Evidence suggests that regular use of high-dose vitamin E may increase the risk of death from all causes by a small amount. These conclusions have been criticized by some experts. Nonetheless, this is the best available scientific evidence currently. Chronic use of vitamin E should be used cautiously, and high-dose vitamin E should be avoided. Acute overdose of vitamin E is very uncommon.
In rare cases, vitamin E supplementation has been associated with dizziness, fatigue, headache, weakness, blurred vision, abdominal pain, diarrhea, nausea, or flu-like symptoms (particularly when used in high doses). The risk of necrotizing enterocolitis may be increased with large doses of vitamin E.
Use cautiously in patients with cardiovascular conditions. Vitamin E may increase risk of all-cause mortality and incidence of heart failure with doses #8805;400 IU daily for over one year.
Vitamin E should be used cautiously for long periods of time (>10 years) due to a possible increased risk of hemorrhagic stroke.
Use cautiously in patients with skin conditions. Skin reactions, such as contact dermatitis and eczema, have been reported with topical vitamin E preparations, such as ointments or vitamin E-containing deodorants. Pruritus (itching) has been reported following oral supplementation of vitamin E.
Use cautiously in patients with kidney impairment. In rare cases, vitamin E supplementation has been associated with gonadal dysfunction and diminished kidney function.
Use cautiously in patients with Alzheimer’s disease or cognitive decline. In patients with Alzheimer’s disease or cognitive decline, vitamin E has been associated with an increase in falls and syncope (fainting).
Oral vitamin E should be used cautiously in patients with retinitis pigmentosa, as is does not appear to slow visual decline and may be associated with more rapid loss of visual acuity, although the validity of this finding has been questioned.
Use cautiously in patients who smoke. Vitamin E supplementation may transiently increase tuberculosis risk in males who smoke heavily and have high dietary vitamin C intake.
Vitamin E should be used cautiously in preterm infants, due to reports of an increased risk of sepsis. Premature infants should be under strict medical supervision. Decisions regarding vitamin supplementation should be made with the infant’s physician.
Although this has not been well studied in humans, an increased risk of bleeding when used with warfarin (Coumadin®), a blood-thinner, has been noted. However, other studies have not observed a greater incidence of bleeding. Bleeding has been observed in patients given high repeated doses of intravenous all-rac-alpha-tocopherol (synthetic vitamin E). Avoid in patients with bleeding disorders or those taking drugs that may increase the risk of bleeding. Dosing adjustments may be necessary. Reported adverse effects attributed to vitamin E supplementation included minor bleeding and epistaxis (nosebleed).
Avoid doses greater than the RDA in pregnant women, due to a possible increased risk of congenital heart defects in offspring.
Avoid with known allergy/hypersensitivity to products that contain vitamin E. Results from the recently published large SELECT trial (the Selenium and Vitamin E Cancer Prevention Trial) is the largest-ever prostate cancer prevention trial – National Cancer Institute at the National Institutes of health), show that vitamin E supplements (400 IU/day) may harm adult men in the general population by increasing their risk of prostate cancer. Follow-up studies are assessing whether the cancer risk was associated with baseline blood levels of vitamin E and selenium prior to supplementation as well as whether changes in one or more genes might increase a man’s risk of developing prostate cancer while taking vitamin E.
Dosage: Intake recommendations for vitamin E and other nutrients are provided in the Dietary Reference Intakes (DRIs) developed by the Food and Nutrition Board (FNB) at the Institute of Medicine of The National Academies (formerly National Academy of Sciences). DRI is the general term for a set of reference values used to plan and assess nutrient intakes of healthy people. These values, which vary by age and gender, include:
Recommended Dietary Allowance (RDA): average daily level of intake sufficient to meet the nutrient requirements of nearly all (97%-98%) healthy people.
Adequate Intake (AI): established when evidence is insufficient to develop an RDA and is set at a level assumed to ensure nutritional adequacy.
Tolerable Upper Intake Level (UL): maximum daily intake unlikely to cause adverse health effects.
The FNB’s vitamin E recommendations are for d–alpha-tocopherol (d-alpha-tocopherol or d-α-tocopherol) if you want to use vitamin E, do not buy any form but this one, which is the only form maintained in plasma.
RDAs for vitamin E are provided in milligrams (mg) and are listed in the table below. Because insufficient data are available to develop RDAs for infants, AIs were developed based on the amount of vitamin E consumed by healthy breastfed babies.
|
Recommended Dietary Allowances (RDAs) for Vitamin E (Alpha-Tocopherol) |
||||
|
Age |
Males |
Females |
Pregnancy |
Lactation |
|
0-6 months* |
4 mg |
4 mg |
|
|
|
7-12 months* |
5 mg |
5 mg |
|
|
|
1-3 years |
6 mg |
6 mg |
|
|
|
4-8 years |
7 mg |
7 mg |
|
|
|
9-13 years |
11 mg |
11 mg |
|
|
|
14+ years |
15 mg |
15 mg |
15 mg |
19 mg |
*Adequate Intake (AI)
Table 7. RDAs for different age groups with Vitamin E.
At present, the vitamin E content of foods and dietary supplements is listed on labels in international units (IUs), a measure of biological activity rather than quantity. Naturally sourced vitamin E is called d-alpha-tocopherol; the synthetically produced form is dl-alpha-tocopherol (do not buy the dl- form, as it does not work as well as the natural d-α-tocopherol).
Conversion rules are as follows:
To convert from mg to IU: 1 mg of alpha-tocopherol is equivalent to 1.49 IU of the natural form or 2.22 IU of the synthetic form.
To convert from IU to mg: 1 IU of alpha-tocopherol is equivalent to 0.67 mg of the natural form or 0.45 mg of the synthetic form.
Tolerable Upper Intake Levels (ULs) for Vitamin E:
|
Age |
Male |
Female |
Pregnancy |
Lactation |
| 1-3 years |
200 mg |
200 mg |
||
| 4-8 years |
300 mg |
300 mg |
||
| 9-13 years |
600 mg |
600 mg |
||
| 14-18 years |
800 mg |
800 mg |
800 mg |
800 mg |
| 19+ years |
1,000 mg |
1,000 mg |
1,000 mg |
1,000 mg |
Table 8. Tolerable upper limits for Vitamin E at different age levels.
No specific dosing of vitamin E has been established for other conditions, and there is recent evidence suggesting possible adverse health effects from long-term use of daily supplementation with 400 IU or greater daily. Although controversial, the use of long-term vitamin E supplementation should be approached cautiously until further evidence from prospective clinical trials is available. Various doses and durations have been evaluated in clinical trials, although many have not been proven as effective or safe. It is recommended that patients discuss the choice of dosing and duration with their doctors.
This concludes the series of articles about vitamins and supplements in sports and in normal life. If people want to know more about other supplements, they may leave suggestions in the comments section following this article. When there are enough to warrant an article, I will write one and publish it on Fishduck.com.
The next article will be all about head injuries and concussions. We will look at the normal brain and what happens when there is a head injury. We will discuss how concussions happen and what symptoms there are. We will then discuss in some detail the arguments about how dangerous concussions are, and why, and what long-term effects may be expected. After all that, we will explore safety issues and how to prevent or ameliorate the head injuries in the first place.
I have heard fans say things like: “These young players are ‘wusses”. “I have seen no evidence from human studies that concussions are dangerous and harmful”.
We will provide evidence that even the most skeptical fans will find it difficult to deny any longer. Our Duck players, and the youngsters still in grade and high school, deserve as much protection as technology can provide, and with as much wisdom, respect, and compassion as we can summon to keep such injuries to a minimum, and even to get rid of them altogether. In my years of practice, I have seen too many of these problems in youngsters. I have also been a sad witness to more severe problems as football players retire and age. It is a tragedy for otherwise healthy, relatively young men who should have expected many more years of normal life to enjoy.

Figure 3. Ducks’ Great Defense!
Related Articles:
NeuroDocDuck (Dr. Driesen) is a doctor who specializes in neurology, and sports medicine. He is an Oregon alumnus, completing his medical education and training in the UK. He has been both a practicing clinician and professor, a well-known and respected diagnostician, an author, and has appeared on national television.
NeuroDocDuck is active in his profession, and stays current on all new trends in his field. He enjoys golf and loves his Ducks!